
Introduction : DMD is a part of the spectrum of disorders called as Dystrophinopathies. 2 other disorders of this group are: Becker Muscular Dystrophy(BMD) and DMD-associated dilated cardiomyopathy.
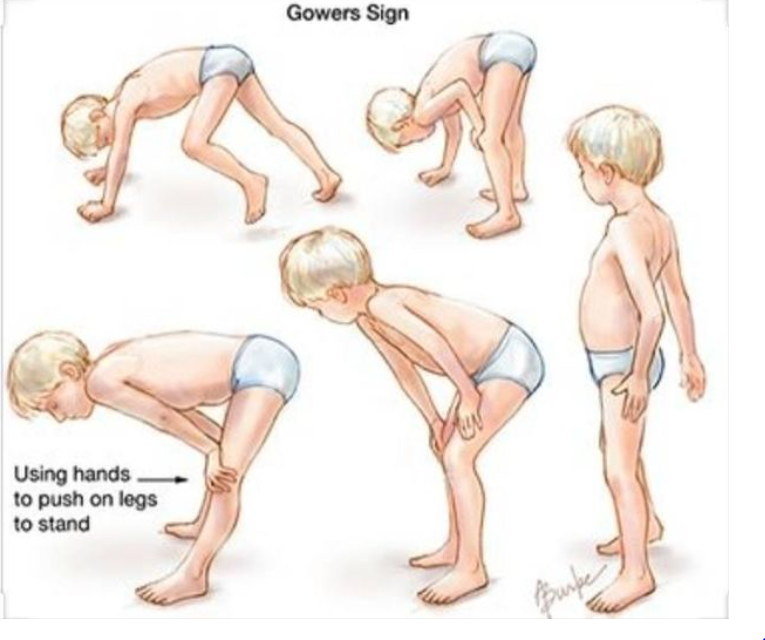
Males with DMD presents , at 2-4 years of age, with progressive muscle weakness. Such individuals are likely to have developmental delay, difficulty in walking, running and getting up from sitting posture. The child usually needs support while rising from sitting/ squatting. A typical Gower’s sign is seen. These children usually become wheel chair bound by 2nd decade of life. They also eventually develop cardiomyopathy and breathing difficulties. Respiratory and cardiac problems often lead to death.
BMD is less severe. Males with BMD present at around 11 years or later. They often survive well into late adulthood with a little less than normal life expectancy. Some of them stay ambulatory even in their 60s. However, some succumb to death in mid 40s. Cardiac complications(Dilated cardiomyopathy) develop because of involvement of the heart muscles.
DMD-associated dilated cardiomyopathy leads to left ventricular dilatation and heart failure. Females who are carriers of a pathogenic DMD gene variants (meaning: a DMD gene variant that has the ability to cause disease) have a higher risk.
Caused by: A defect in the DMD gene.
In males, a hemizygous pathogenic variant cause disease.
Females with a heterozygous pathogenic variant usually does not present with the disease. However, occasionally they may have classic symptoms of muscle weakness and dilated cardiomyopathy.
Inheritance : X linked
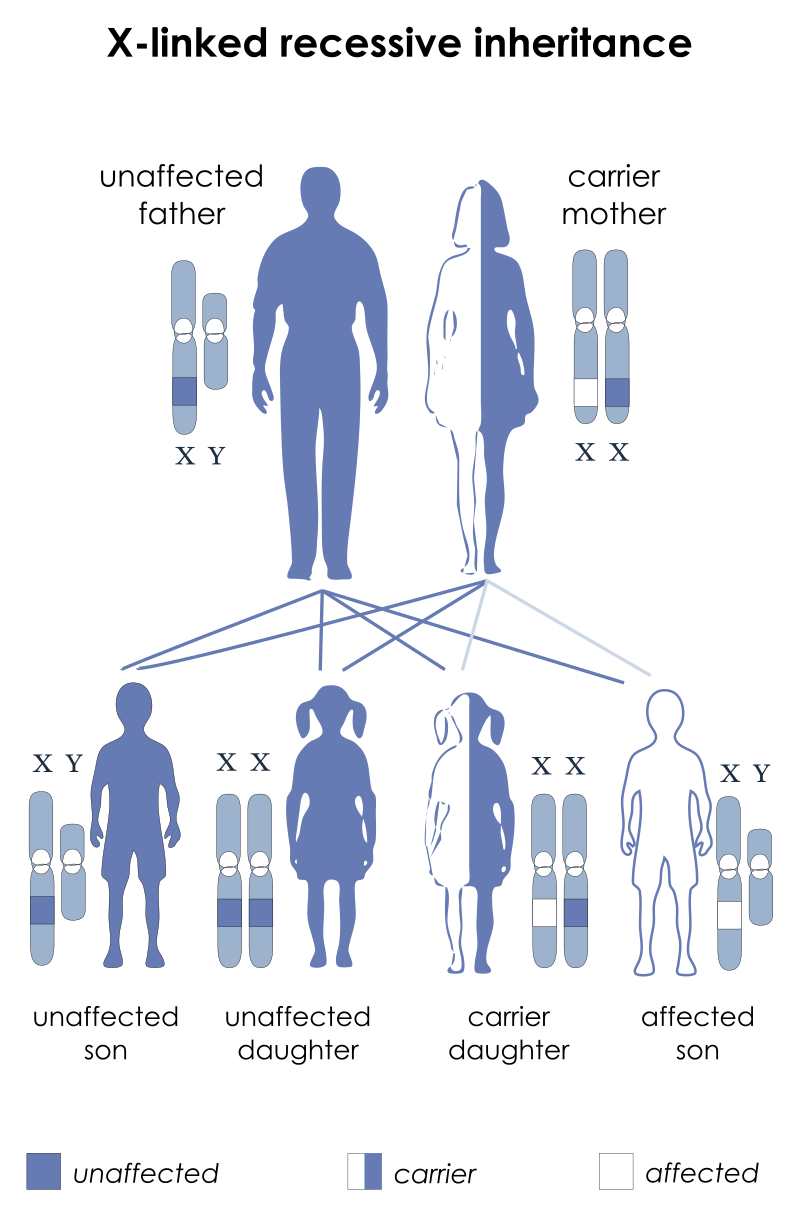
Recurrence risk : There is a 50% chance that a heterozygous female(carrier) will transmit a pathogenic DMD gene variant in each pregnancy. If a son inherits the pathogenic DMD gene variant, he will be affected. However, if a daughter inherits the pathogenic variant, she may or may not present with disease.
A male, affected with BMD or DMD-associated dilated cardiomyopathy, will transmit a pathogenic DMD gene variant to his all his daughters. However, his sons will not inherit the gene variant.
Frequency: DMD: 1 in 3500 males approximately. BMD: 1 in 20000 males approximately.
Management:
Multidisciplinary approach is required (Neurology, Physiotherapy, Physical Medicine and Rehabilitation, Cardiology)
Corticosteroids help to improve muscle strength in DMD.
Immunizations for respiratory infections(Pneumococcus, Influenza)
Nutritional assessment. A balanced diet is essential. Avoid obesity.
Vitamin D and Calcium supplements to maintain bone density and prevent fractures.
Avoid exposure to botulinum toxin, succinylcholine and inhalational anesthetic agents(May cause Malignant hyperthermia)
Surveillance:
Cardiac evaluation : Annually or half yearly.
Pulmonary function evaluation: Annually or half yearly.
Physical Medicine and rehabilitation : Monitor for scoliosis (spine deformity) and contractures.
Information curated by: Dr Sweta Das.
For further references:-
https://www.ncbi.nlm.nih.gov/books/NBK1119/
https://www.omim.org/entry/310200
Date: 16/12/2021


